Kawasaki Disease in a 4-Year-Old: Diagnosis, Criteria & Management | NEET SS
In this case, the echocardiographic finding is not merely “coronary dilatation”; an LAD Z-score of +2.8 falls into the small coronary artery aneurysm category. This distinction is important for NEET SS because Kawasaki disease is the most common cause of acquired heart disease in children in developed countries, and coronary artery aneurysm is its most important complication.
Arjun, a previously healthy 4-year-old boy, is brought to the paediatric emergency because fever has persisted despite antipyretics. Through this case, we will approach history, examination, investigations, differential diagnosis, incomplete Kawasaki disease, acute management, IVIG resistance, coronary Z-score interpretation, and NEET SS-focused MCQs.
Presenting Complaint
“My son has had a fever for 6 days. His eyes look very red, his lips are dry and cracked, his tongue is bright red, and there is a swelling on one side of his neck. He also has a red rash over his body, and his hands and feet look swollen.”
Arjun, a 4-year-old boy, is brought by his mother to the Paediatric Emergency Department of a tertiary care centre.
Fig1.
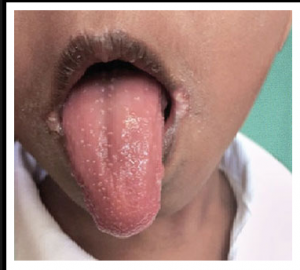
Fig2.

History of Presenting Complaint
Q1. When did the fever start, and how high has it been?
Ans – The fever started 6 days ago and has been present every day. It is usually high-grade, around 102–103°F and comes down only partially after paracetamol. He becomes irritable whenever the fever rises.
Q2. Did you notice redness of the eyes? Was there discharge?
Ans – Both eyes became red from the third day of fever. There is no sticky discharge, no pus, and his eyelids are not stuck together in the morning.
Q3. When did the rash appear, and where did it start?
Ans – The rash appeared on the fourth day. It started over the trunk and then involved the limbs. It is red and patchy. There are no blisters, no blackish spots, and he is not scratching it much.
Q4. What changes did you notice in the mouth?
Ans – His lips became very red and cracked. His tongue looks unusually red and rough. He is drinking less because his mouth appears sore.
Q5. Tell me about the neck swelling.
Ans – The swelling appeared 2 days ago on the right side of the neck. It is tender, about 2 cm in size, and there is no pus discharge.
Q6. Any cough, cold, vomiting, diarrhoea, joint pain, or drowsiness?
Ans – There is no cough, no significant cold, no repeated vomiting, no joint swelling, no drowsiness, and no seizures. He passed loose stool once but is otherwise passing urine.
Q7. Any recent illness, drug intake, sick contact, or travel?
Ans – There is no recent travel, no similar illness in school or at home, and no new medicine apart from paracetamol.
Clinical Teaching Point: In a fever with rash and conjunctival congestion, vaccination history is essential because measles is an important differential. However, bilateral non-purulent conjunctivitis, oral mucosal inflammation, extremity oedema, cervical lymphadenopathy, and sterile inflammatory markers strongly favour Kawasaki disease.
Other Parts of History
| Label | Content |
| Past Medical History | Previously healthy; no congenital heart disease, recurrent infections, or autoimmune disorders. |
| Drug History | Has taken only oral paracetamol; no antibiotics, anticonvulsants, sulfonamides, or other new medications. |
| Vaccination History | Immunisations are up to date for age, including the measles vaccine. |
| Family History | No family history of vasculitis, autoimmune disease, recurrent fever syndromes, or early coronary disease. |
| Social History | School-going child living with parents and a sibling; the sibling is well, and there is no fever or rash at home. |
| Allergy History | No known drug allergies. |
Important Diagnoses to Rule Out Before Examination
| Diagnosis | Why it must be considered, and what would clinch it |
| Bacterial sepsis/meningococcaemia | High-grade fever with rash can indicate invasive bacterial disease; toxic appearance, shock, purpura, altered sensorium, or positive cultures would clinch it. |
| Measles | Fever, conjunctival redness, mucosal involvement, and rash overlap; cough-coryza-conjunctivitis, Koplik spots, cephalocaudal rash, and incomplete immunisation would support measles. |
| Scarlet fever | Fever, rash, and strawberry tongue may mimic Kawasaki disease; exudative tonsillitis, sandpaper rash, Pastia lines, and streptococcal evidence would favour it. |
| Systemic JIA | Prolonged fever with rash may resemble inflammatory vasculitis; quotidian fever, evanescent salmon-pink rash, arthritis, hepatosplenomegaly, and hyperferritinaemia would support it. |
Clinical Examination
Part A — Vitals
| Parameter | Value | Interpretation |
| Temperature | 39.2°C | Persistent high-grade fever |
| Heart rate | 138/min | Tachycardia, partly fever-related |
| Respiratory rate | 28/min | Mild tachypnoea |
| Blood pressure | 92/58 mmHg | Preserved perfusion; no shock |
| SpO₂ | 99% on room air | Normal oxygenation |
| Weight | 16 kg | Required for IVIG and aspirin dose calculation |
Part B — Systemic Examination
- General appearance: Febrile, irritable, uncomfortable child; not toxic, no meningeal signs, capillary refill <2 seconds.
- Eyes: Bilateral bulbar conjunctival injection without purulent discharge.
- Oral cavity: Erythematous cracked lips, strawberry tongue, and diffuse oropharyngeal erythema.
- Skin: Generalised polymorphous erythematous maculopapular rash, non-vesicular and non-petechial.
- Extremities: Erythema and oedema of palms and soles, with tenderness during handling; no periungual desquamation yet.
- Neck: Right anterior cervical lymph node approximately 2 cm, tender, non-fluctuant.
- Cardiovascular system: Tachycardia, normal heart sounds, no murmur, gallop, hepatomegaly, or signs of congestive cardiac failure.
- Respiratory system: Bilateral equal air entry; no crepitations or wheeze.
- Abdomen: Soft, non-tender, no hepatosplenomegaly.
- CNS: Conscious, irritable, consolable, no focal neurological deficit.
AHA Criteria Checklist:
- ü Fever ≥5 days
- ü Bilateral non-exudative conjunctivitis
- ü Oral mucosal changes
- ü Polymorphous rash
- ü Extremity changes
- ü Cervical lymphadenopathy ≥1.5 cm
Investigations
| Test | Result | Normal Range | Clinical Significance |
| Haemoglobin | 10.8 g/dL | 11.5–13.5 g/dL | Mild anaemia of inflammation |
| Total leukocyte count | 17,800/mm³ | 5,000–15,000/mm³ | Neutrophilic leukocytosis |
| Platelet count | 5.8 lakh/mm³ | 1.5–4.5 lakh/mm³ | Thrombocytosis; classically prominent after the first week |
| ESR | 82 mm/hr | <20 mm/hr | Significant systemic inflammation |
| CRP | 96 mg/L | <5 mg/L | Markedly elevated; risk marker for severe inflammation |
| Serum albumin | 2.8 g/dL | 3.5–5.0 g/dL | Hypoalbuminaemia: a poor prognostic marker |
| Serum sodium | 132 mmol/L | 135–145 mmol/L | Mild hyponatraemia associated with an inflammatory burden |
| ALT | 86 IU/L | <40 IU/L | Hepatic inflammatory involvement |
| Urine routine | Sterile pyuria | Absent | Supports Kawasaki disease when the urine culture is negative |
| 2D echocardiography | LAD coronary artery Z-score +2.8 | Z-score <+2.0 | Small coronary artery aneurysm; most important baseline investigation |
Coronary artery assessment is central to diagnosis, risk stratification, and follow-up. A Z-score of +2.8 should be classified as a small coronary artery aneurysm, not merely coronary dilatation.
AHA-style Z-score interpretation:
| Coronary Z-score | Interpretation |
| <2.0 | No coronary involvement |
| 2.0 to <2.5 | Dilatation only |
| ≥2.5 to <5.0 | Small coronary artery aneurysm |
| ≥5.0 to <10.0 | Medium coronary artery aneurysm |
| ≥10.0 or absolute dimension ≥8 mm | Giant coronary artery aneurysm |
Diagnosis
Classic Kawasaki Disease with Small Left Anterior Descending Coronary Artery Aneurysm, LAD Z-score +2.8.
This is classic Kawasaki disease because the child has fever for ≥5 days with all five principal clinical criteria: bilateral non-exudative conjunctivitis, oral mucosal changes, polymorphous rash, extremity changes, and cervical lymphadenopathy. The echocardiographic LAD Z-score of +2.8 confirms small coronary artery aneurysmal involvement, rather than simple coronary dilatation. For NEET SS, this case is high yield because diagnosis is clinical, but risk stratification and follow-up depend heavily on coronary Z-score classification.
Differentials Explained — Why Each Was Ruled Out
| Differential | Features Suggesting It | Features Against It | Verdict |
| Viral exanthem, EBV / adenovirus | Fever, rash, conjunctival redness | No exudative pharyngitis, no hepatosplenomegaly, small LAD coronary aneurysm present | RULED OUT |
| Bacterial lymphadenitis | Tender unilateral cervical lymph node | Multisystem mucocutaneous findings and sterile pyuria favour KD | RULED OUT |
| Scarlet fever | Fever, rash, strawberry tongue | No exudative tonsillitis, no sandpaper rash, no Pastia lines | RULED OUT |
| Stevens-Johnson syndrome | Fever with mucosal involvement | No target lesions, bullae, epidermal necrolysis, or drug trigger | RULED OUT |
| Systemic JIA | Prolonged fever and rash | No arthritis, no quotidian fever, rash not salmon-pink or evanescent | RULED OUT |
| Kawasaki Disease | Fever ≥5 days, all AHA criteria, high inflammatory markers, LAD Z-score +2.8 small coronary aneurysm | No stronger alternative diagnosis | CONFIRMED |
Management
Phase 1 — Acute Phase: First 24–48 Hours
Admit the child for close paediatric and cardiac monitoring. Start intravenous immunoglobulin, IVIG 2 g/kg IV as a single infusion over 10–12 hours. For Arjun, weighing 16 kg, the total dose is 32 g IV once. Monitor temperature, heart rate, blood pressure, urine output, infusion reactions, and clinical features of myocarditis or cardiac failure.
ASPIRIN DOSE:
Start aspirin 30–50 mg/kg/day orally in 4 divided doses during the acute febrile inflammatory phase. For a 16 kg child, this corresponds to a total daily dose of 480–800 mg/day, divided every 6 hours, approximately 120–200 mg per dose every 6 hours.
Avoid ibuprofen because it may interfere with aspirin’s antiplatelet action. Monitor for gastrointestinal irritation, hepatic dysfunction, bleeding tendency, and symptoms suggestive of salicylate toxicity.
Phase 2 — Subacute Phase: After Fever Resolution
After the child remains afebrile for 48–72 hours, reduce aspirin to an antiplatelet dose: 3–5 mg/kg/day orally once daily. For Arjun, this is approximately 50–80 mg once daily. Repeat echocardiography around 2 weeks, monitor platelet count, and advise avoidance of strenuous activity until the coronary status is reassessed.
Because this child has a small coronary artery aneurysm, antiplatelet therapy and cardiology follow-up should be continued according to serial echocardiographic findings.
Phase 3 — IVIG-Resistant Kawasaki Disease
IVIG resistance is defined as persistent or recrudescent fever ≥36 hours after completion of IVIG. Treatment options include repeat IVIG 2 g/kg IV once or infliximab 5 mg/kg IV once. Corticosteroids may be considered in refractory disease or high-risk inflammatory phenotypes under specialist supervision.
Long-Term Follow-Up
Repeat echocardiography at 6–8 weeks. Continue antiplatelet therapy according to coronary status. Defer live vaccines such as MMR and varicella for 11 months after IVIG. Giant coronary aneurysms require paediatric cardiology-led antithrombotic therapy, often including antiplatelet plus anticoagulation.
Pharmacology Management
The preferred IVIG regimen is 2 g/kg as a single infusion, not the older divided 5-day schedule. Aspirin is one of the few accepted indications for aspirin use in children. In this revised case, the acute aspirin dose is written as 30–50 mg/kg/day in 4 divided doses, followed by antiplatelet aspirin 3–5 mg/kg/day once daily after defervescence. Early IVIG is the most effective therapy for preventing coronary complications.
NEET SS Rapid Revision
| Rapid Revision Point | High-Yield Answer |
| The most common cause of acquired heart disease in children in developed countries | Kawasaki disease |
| Most important complication | Coronary artery aneurysm |
| Most important investigation | 2D echocardiography |
| Most effective therapy for preventing coronary complications | IVIG 2 g/kg IV once |
| Aspirin in children | One of the few accepted paediatric indications for aspirin use |
| IVIG-resistant Kawasaki disease | Persistent or recurrent fever ≥36 hours after IVIG completion |
| Coronary Z-score ≥2.5 | Aneurysmal coronary involvement |
| LAD Z-score +2.8 in this case | Small coronary artery aneurysm |
NEET SS MCQ
Q1. A 4-year-old child presents with fever for 6 days, bilateral non-purulent conjunctivitis, cracked lips, strawberry tongue, polymorphous rash, extremity oedema, and cervical lymphadenopathy. Which is the single most important investigation at diagnosis?
a. Throat swab culture
b. 2D echocardiography
c. Serum ferritin
d. Anti-streptolysin O titre
Correct answer: b. 2D echocardiography
Explanation: Kawasaki disease is primarily a clinical diagnosis, but echocardiography is mandatory at baseline to evaluate coronary artery involvement. It is the key investigation for detecting coronary dilatation or aneurysm and for planning follow-up.
Q2. A child with classic Kawasaki disease receives IVIG 2 g/kg but remains febrile 48 hours after completion of infusion. What is the next appropriate step?
a. Stop aspirin immediately
b. Repeat IVIG 2 g/kg or administer infliximab 5 mg/kg
c. Start oral amoxicillin-clavulanate only
d. Give the MMR vaccine before discharge
Correct answer: b. Repeat IVIG 2 g/kg or administer infliximab 5 mg/kg
Explanation: Fever persisting ≥36 hours after IVIG indicates IVIG-resistant Kawasaki disease. Repeat IVIG or infliximab is an accepted escalation strategy. Antibiotics alone do not treat coronary vasculitis, and live vaccines should be deferred after IVIG.
Q3. How long should MMR vaccination be deferred after IVIG therapy for Kawasaki disease?
a. 4 weeks
b. 3 months
c. 6 months
d. 11 months
Correct answer: d. 11 months
Explanation: IVIG may neutralise live attenuated vaccine virus and impair vaccine immunogenicity. Therefore, MMR and varicella vaccines are generally deferred for 11 months after IVIG therapy in Kawasaki disease.
Q4. A 4-year-old child with Kawasaki disease has an LAD coronary artery Z-score of +2.8 on echocardiography. How should this be classified?
a. Normal coronary artery
b. Coronary dilatation only
c. Small coronary artery aneurysm
d. Giant coronary artery aneurysm
Correct answer: c. Small coronary artery aneurysm
Explanation: Coronary Z-score ≥2.5 to <5.0 is classified as a small coronary artery aneurysm. Therefore, LAD Z-score +2.8 should not be described as simple dilatation.
References
1. Gupta P, Menon PSN, Ramji S, Lodha R, editors. PG Textbook of Pediatrics. 3rd ed. New Delhi: Jaypee Brothers Medical Publishers; 2022.
2. Gupta P. UG Textbook of Pediatrics. New Delhi: Jaypee Brothers Medical Publishers; 2023.
3. Gupta P, Bedi N. Pediatric Drug Formulary. New Delhi: Jaypee Brothers Medical Publishers; 2023.
4. Kumar R, Ratageri V, Gupta P. IAP Standard Treatment Guidelines. New Delhi: Jaypee Brothers Medical Publishers.
5. Ghai OP, Gupta P, Paul VK. Ghai Essential Pediatrics. New Delhi: CBS / Jaypee-associated pediatric academic reference editions where applicable; use Jaypee edition only if available in your institutional library.