: A High-Yield Topic for NEET PG 2026")
Traumatic Brain Injury (TBI): A High-Yield Topic for NEET PG 2026
Traumatic Brain Injury (TBI) is important topic for medical students and is often tested in entrance exams like NEET PG due to its clinical significance and high incidence in emergency medicine. This comprehensive overview covers everything you need to know from classification and pathology to neuropsychiatric consequences plus helpful checklist at the end to ensure you’re ready for exam day.
Classification of TBI
The American Academy of Neurology typically classifies TBI into two broad categories: Moderate and Severe but most clinical and exam-related references divide TBI into three categories based on the Glasgow Coma Scale (GCS):
| Severity | GCS Score | Clinical Features |
| Mild TBI (Concussion) | 13–15 | May have brief (<30 min) loss of consciousness or confusion; no focal neuro deficits; amnesia < 24 hrs |
| Moderate TBI | 9–12 | Prolonged unconsciousness; possible focal neurological signs |
| Severe TBI | ≤8 | Loss of consciousness >12 hrs; often with structural brain damage (seen on imaging) and neurological deficits |
History & Milestones in TBI
- Earliest Evidence: TBI evidence from a skull in South Africa dates fpr 1 million years.
- First Written Record: Found in the Edwin Smith Papyrus (500 years ago) detailing cranial injuries.
- Phineas Gage Case: A railroad worker whose personality drastically changed after a frontal lobe injury classic case demonstrating the brain behaviour relationship.
Pathophysiology of TBI
TBI can be classified based on:
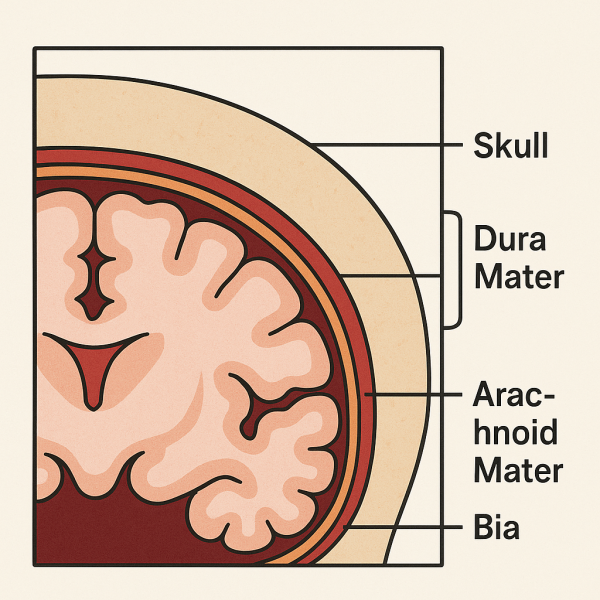
- Integrity of Meningeal Coverings
- Closed TBI: Skull intact; more common (falls, car accidents).
- Penetrating TBI: Skull and meninges breached (missile injuries, blasts in combat zones).
- Timing of Injury
- Primary Injury: Direct result of trauma (contusions, skull fractures, coup/contrecoup injuries, DAI).
- Secondary Injury: Due to physiological processes after injury (ischemia, hypoxia, edema, infections).
- Type of Lesion
- Focal Lesions: Contusions, hemorrhages, lacerations—often at frontal/temporal poles.
- Diffuse Lesions:
- Traumatic Axonal Injury (TAI): Shearing forces disrupt axonal pathways (corpus callosum, brainstem).
- Diffuse Ischemic Damage (DID): Often from hypoxia or vascular insult after injury.
Types of Intracranial Hemorrhages
| Type | Cause | Location | Imaging Appearance | Key Features |
| Epidural Hematoma | Temporal bone fracture; middle meningeal artery tear | Between skull and dura | Biconvex (lens-shaped); hyperdense | Lucid interval; rapid deterioration |
| Subdural Hematoma | Tearing of bridging veins | Between dura and arachnoid | Crescent-shaped | More common in elderly; chronic SDH mimics dementia |
| Subarachnoid Hemorrhage | Trauma or ruptured aneurysm | Between arachnoid and pia | Blood in sulci/CSF spaces | Thunderclap headache, meningeal signs |
Neuropsychiatric Consequences
| Acute Syndromes | Delayed (Chronic) Syndromes |
| Confusion, agitation, amnesia, delirium | Traumatic dementia, organic personality disorder, Pseudobulbar affect (PBA), anosognosia |
Epidemiology & Risk Factors (Kaplan & Sadock, 9th Ed.)
- Incidence:
- 80% Mild TBI
- 10% Moderate
- 10% Severe
- Age: Highest in adolescents and young adults; second most affected group is the elderly.
- Gender: Males are 40% more likely to suffer TBI.
- Common Causes:
- Falls – most common overall
- Car crashes & assaults – younger individuals
- Sports injuries
- Blast injuries – military personnel
- Risk Factors:
- Alcohol and drug abuse
- History of prior TBI
- Low socioeconomic status
- Ethnicity (higher rates among African Americans)
Clinical Pearls & Mnemonics
- PAD for Meninges: Pia, Arachnoid, Dura (inside to out).
- Coup vs. Contrecoup: Direct vs. opposite side of impact.
- Lucid interval = Think Epidural Hematoma
- Chronic SDH = “Reversible dementia” in elderly
TBI is not just a high-yield topic for exams like NEET PG Exam, it’s also a cornerstone of clinical neurology, emergency medicine, and psychiatry. A good grasp of its classifications, clinical features, and complications can help you crack even the trickiest MCQs.
Frequently Asked Questions:
1. Can you fully recover from a brain injury?
Most studies suggest that once brain cells are destroyed or damaged, for the most part, they do not regenerate. However, recovery after brain injury can take place, especially in younger people, as, in some cases, other areas of the brain make up for the injured tissue.
2. What are the symptoms of traumatic brain injury?
Moderate to severe traumatic brain injuries
- Loss of consciousness from several minutes to hours.
- Persistent headache or headache that worsens.
- Repeated vomiting or nausea.
- Convulsions or seizures.
- Dilation of one or both pupils of the eyes.
- Clear fluids draining from the nose or ears.
- Inability to awaken from sleep.
3. What is the recovery time for a TBI?
Traumatic brain injury (TBI) recovery time varies greatly depending on the severity of the injury, but generally, the most rapid recovery occurs within the first 3-6 months post-injury. While many regain consciousness within the first year after a TBI, some may continue to experience slow recovery for several years, especially those with severe injuries.