Retinal Diseases in MD Ophthalmology: A Complete Guide for PG Residents
Retinal diseases form one of the most important areas of MD Ophthalmology training. From diabetic retinopathy and retinal detachment to age-related macular degeneration and vitreoretinal surgery, retina is a high-yield subject for university exams, clinical postings, case discussions and future sub-speciality practice.
For an ophthalmology resident, mastering retinal diseases is not just about memorising classifications. It requires a strong understanding of retinal anatomy, fundus interpretation, imaging, laser principles, intravitreal therapy and surgical decision-making. Retinal conditions are also frequently tested in PG ophthalmology exams because they combine clinical examination, emergency diagnosis and long-term disease management.

What Are Retinal Diseases? Overview for Ophthalmology PG Students
Retinal diseases are disorders affecting the neurosensory retina, retinal pigment epithelium, retinal vasculature, macula, vitreoretinal interface or choroid-retina complex. These conditions may be vascular, degenerative, inflammatory, genetic, traumatic or surgical in nature.
Common examples include diabetic retinopathy, retinal detachment, retinal vein occlusion, central retinal artery occlusion, age-related macular degeneration, retinitis pigmentosa, macular hole and epiretinal membrane.
For residents, retina is a clinically demanding branch because many diseases require rapid recognition. A missed retinal detachment, uncontrolled proliferative diabetic retinopathy or untreated wet ARMD can lead to irreversible visual loss.
Anatomy of the Retina: What Every MD Ophthalmology Resident Must Know
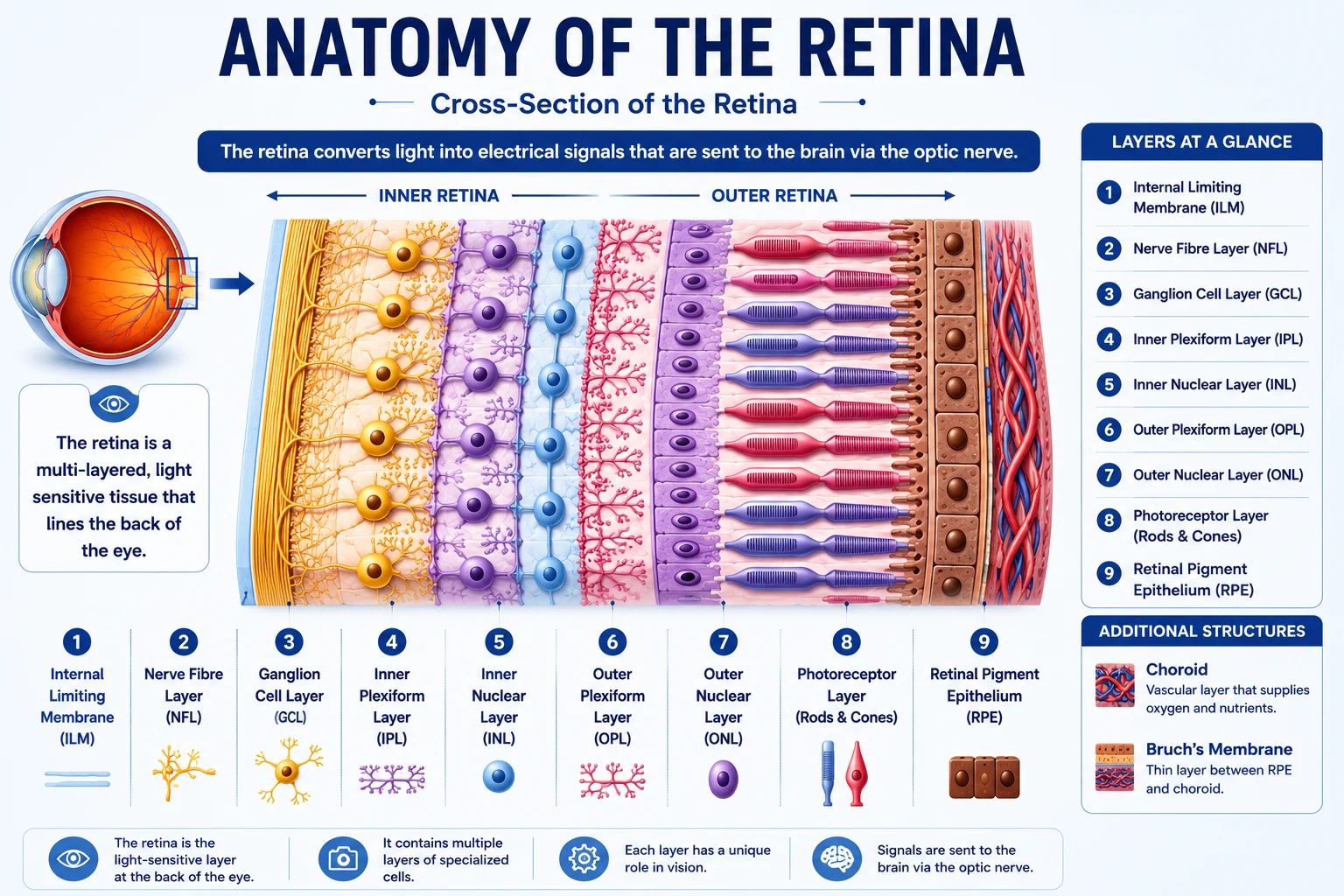
The retina is a thin, multilayered neural tissue lining the posterior segment of the eye. Important layers include the internal limiting membrane, nerve fibre layer, ganglion cell layer, inner plexiform layer, inner nuclear layer, outer plexiform layer, outer nuclear layer, photoreceptor layer and retinal pigment epithelium.
The macula is responsible for central vision, with the fovea providing the highest visual acuity. The optic disc marks the exit of retinal nerve fibres, while the retinal vessels provide clues to vascular and systemic diseases. The vitreous, though not part of the retina, plays a major role in posterior vitreous detachment, retinal tears, vitreous haemorrhage and tractional retinal diseases.
A resident must be comfortable identifying the disc, macula, retinal vessels, peripheral retina, retinal breaks, haemorrhages, hard exudates, cotton wool spots, drusen, neovascularisation and areas of traction.
Why Retinal Diseases Are Critical in Your Residency Training
Retinal diseases are critical because they are common, vision-threatening and clinically testable. They also require integration of multiple skills: indirect ophthalmoscopy, slit-lamp biomicroscopy, fundus photography, OCT, fluorescein angiography and B-scan ultrasonography.
Retina cases are often included in practical examinations because they allow examiners to assess diagnosis, staging, systemic association, investigation choice and management planning. For residents revising ophthalmology basics, topics such as diabetic retinopathy, retinal detachment and macular diseases should be studied along with other Important Topics Ophthalmology MBBS.
Diabetic Retinopathy: The Most Common Retinal Disease in India
Diabetic retinopathy is one of the most important retinal diseases for MD Ophthalmology residents. India has a large diabetic population, making diabetic retinopathy a major cause of preventable visual impairment. A Lancet Global Health study highlighted the need for national and subnational estimates of diabetic retinopathy in India to support retinal screening and blindness prevention strategies.
Classification: Non-Proliferative vs Proliferative Diabetic Retinopathy
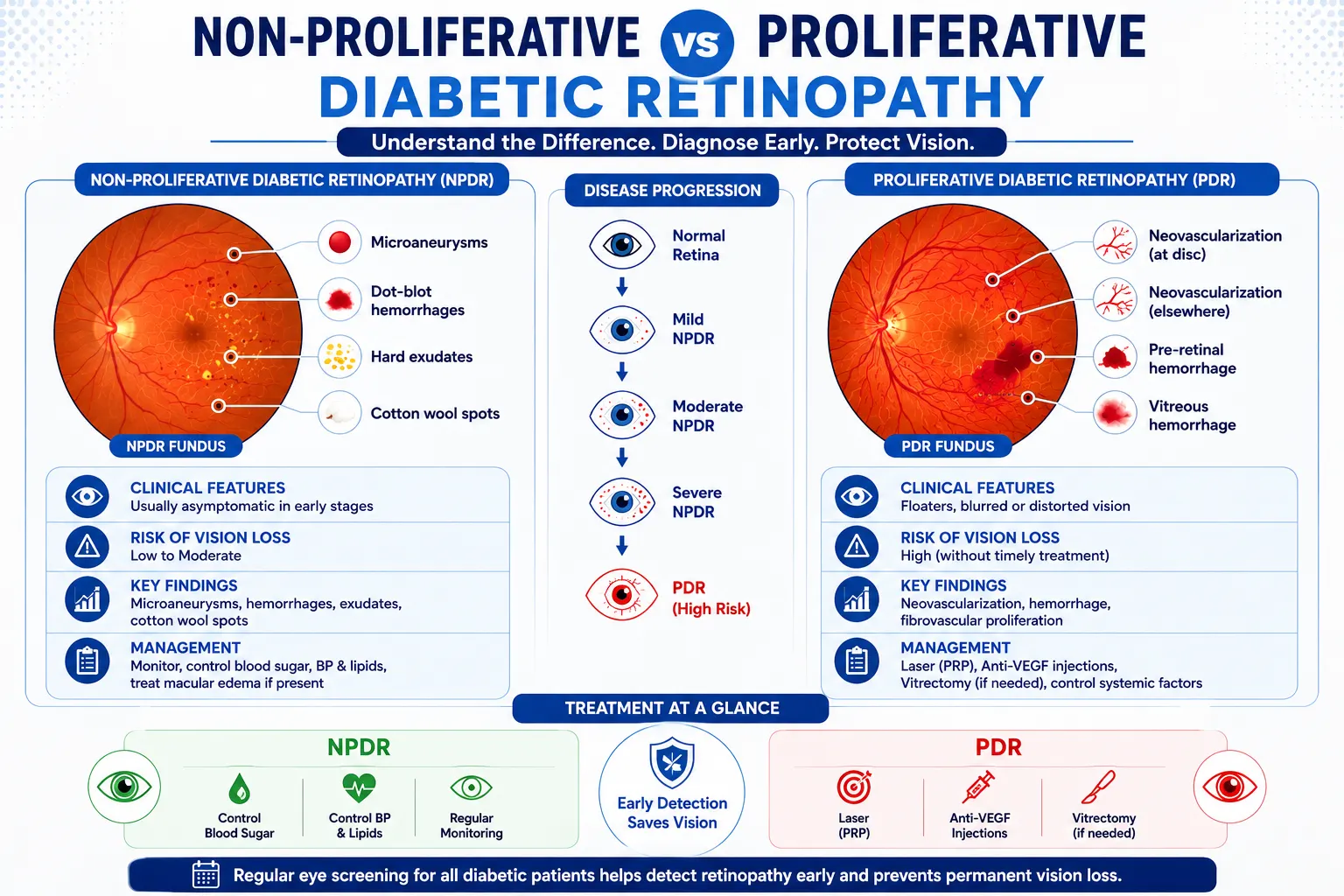
Diabetic retinopathy is broadly classified into non-proliferative diabetic retinopathy and proliferative diabetic retinopathy.
Non-proliferative diabetic retinopathy includes microaneurysms, dot-blot haemorrhages, hard exudates, cotton wool spots, venous beading and intraretinal microvascular abnormalities. It may be mild, moderate, severe or very severe depending on the extent of retinal changes.
Proliferative diabetic retinopathy is characterised by neovascularisation at the disc or elsewhere. These fragile new vessels may bleed, leading to vitreous haemorrhage, fibrovascular proliferation and tractional retinal detachment.
Diabetic macular oedema can occur at any stage and is a major cause of visual loss in diabetic patients.
Clinical Features and Fundus Findings You Must Recognise
Patients may be asymptomatic in early stages. As the disease progresses, they may complain of blurred vision, floaters, sudden visual loss, difficulty reading or reduced central vision.
Fundus findings include microaneurysms, retinal haemorrhages, hard exudates, macular oedema, cotton wool spots, venous beading, IRMA, neovascularisation, pre-retinal haemorrhage, vitreous haemorrhage and tractional retinal detachment.
Residents must learn to identify clinically significant macular oedema, proliferative changes and high-risk PDR because these findings directly influence treatment decisions.
Management of Diabetic Retinopathy: Laser, Anti-VEGF and Surgery
Management depends on the stage of disease, presence of macular oedema and level of proliferative activity. Systemic control of blood glucose, blood pressure and lipids is essential, but ophthalmic treatment is required when vision-threatening retinopathy develops.
The American Academy of Ophthalmology’s Diabetic Retinopathy Preferred Practice Pattern states that anti-VEGF agents are effective for centre-involved diabetic macular oedema with vision loss, reduce severity of diabetic retinopathy and treat proliferative diabetic retinopathy. It also notes that panretinal photocoagulation remains an important treatment for PDR.
Laser Photocoagulation: When and How to Use It
Laser photocoagulation is used mainly for proliferative diabetic retinopathy and selected cases of macular oedema. Panretinal photocoagulation reduces the ischemic drive for neovascularisation. Focal or grid laser may be used in selected macular oedema cases depending on clinical and imaging findings.
Residents must understand laser settings, spot size, duration, burn intensity and the complications of excessive laser, including visual field loss and reduced night vision.
Anti-VEGF Injections: Indications and Agents
Anti-VEGF therapy is widely used in diabetic macular oedema, PDR, retinal vein occlusion and wet ARMD. Common agents include bevacizumab, ranibizumab and aflibercept. The American Academy of Ophthalmology lists wet AMD, macular oedema, diabetic retinopathy and retinal vein occlusion among eye conditions treated with anti-VEGF medicines.
For residents, it is important to know injection technique, indications, contraindications, consent, asepsis and complications such as endophthalmitis, raised IOP and intraocular inflammation.
Pars Plana Vitrectomy for Advanced Diabetic Retinopathy
Pars plana vitrectomy is indicated in non-clearing vitreous haemorrhage, tractional retinal detachment threatening or involving the macula, combined tractional-rhegmatogenous retinal detachment and dense premacular haemorrhage.
The aim is to remove vitreous haemorrhage, relieve traction, dissect fibrovascular membranes, apply endolaser and stabilise the retina using tamponade when required.
Retinal Detachment: Diagnosis and Emergency Management
Retinal detachment is an ophthalmic emergency. Delay in diagnosis can result in permanent visual loss, especially when the macula is involved.
-
Types of Retinal Detachment: Rhegmatogenous, Tractional and Exudative
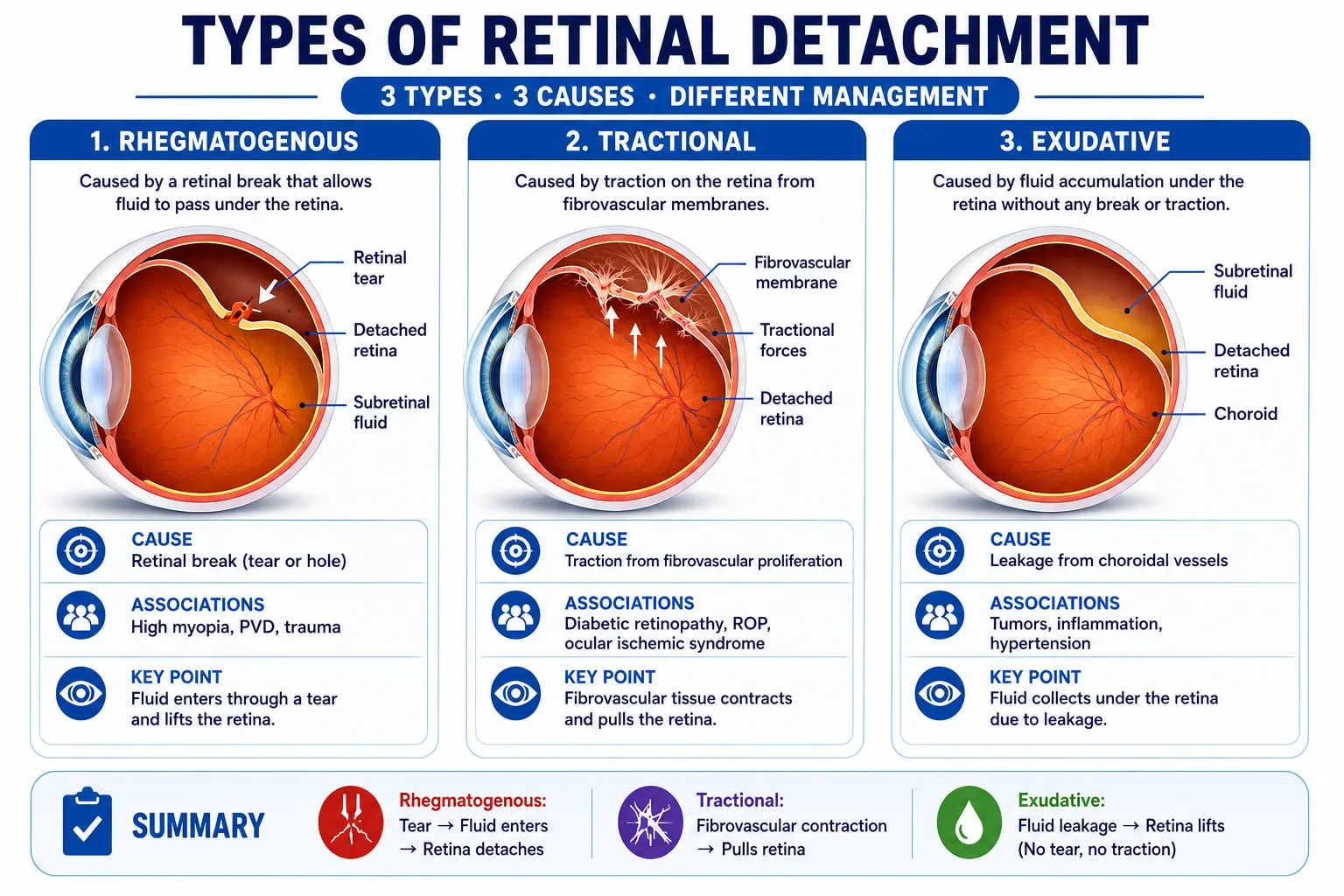
Rhegmatogenous retinal detachment occurs due to a retinal break that allows fluid to pass into the subretinal space. It is commonly associated with posterior vitreous detachment, lattice degeneration, high myopia, trauma or previous intraocular surgery.
Tractional retinal detachment occurs when fibrovascular membranes pull the retina away from the retinal pigment epithelium. It is commonly seen in proliferative diabetic retinopathy.
Exudative retinal detachment occurs due to fluid accumulation under the retina without a retinal break, often because of inflammatory, vascular or neoplastic causes.
-
Symptoms, Signs and Fundoscopy Findings
Symptoms include sudden-onset floaters, flashes of light, a curtain-like shadow, peripheral field loss and reduced vision if the macula is detached.
Fundoscopy may show an elevated, grey, mobile retina in rhegmatogenous retinal detachment. Retinal breaks, horseshoe tears, lattice degeneration, subretinal fluid and pigment cells in the anterior vitreous may be seen.
-
Surgical Treatment: Scleral Buckling, Vitrectomy and Pneumatic Retinopexy
Treatment options include laser retinopexy, pneumatic retinopexy, scleral buckling, pars plana vitrectomy or a combination of procedures. EyeWiki by the American Academy of Ophthalmology lists laser retinopexy, pneumatic retinopexy, scleral buckle and vitrectomy among techniques used for retinal detachment repair.
-
When to Choose Scleral Buckling vs Vitrectomy
Scleral buckling is often preferred in selected young phakic patients, anterior breaks, lattice-related detachments and cases where external support can close the break effectively.
Vitrectomy is preferred in posterior breaks, pseudophakic retinal detachment, media opacity, giant retinal tears, proliferative vitreoretinopathy and complex detachments. A recent review notes that scleral buckling, vitrectomy and pneumatic retinopexy have all been used successfully for rhegmatogenous retinal detachment, with choice depending on multiple case-related factors.
-
Post-Operative Care and Complications to Watch
Post-operative care includes positioning advice, monitoring intraocular pressure, checking retinal attachment, identifying infection and ensuring follow-up. Complications include recurrent retinal detachment, proliferative vitreoretinopathy, cataract progression, raised IOP, hypotony, endophthalmitis and epiretinal membrane formation.
-
Age-Related Macular Degeneration: Dry vs Wet
Age-related macular degeneration affects the macula and is an important cause of central visual loss in elderly patients. It is classified into dry and wet forms.
Dry ARMD: Pathophysiology, Drusen and Management
Dry ARMD is characterised by drusen, retinal pigment epithelial changes and geographic atrophy in advanced cases. Patients may complain of gradual central vision decline, difficulty reading and distortion.
Management includes lifestyle modification, smoking cessation, nutritional advice, AREDS-based supplementation in selected patients and regular monitoring for conversion to wet ARMD.
Wet ARMD: CNV, Intravitreal Injections and Monitoring
Wet ARMD is caused by choroidal neovascularisation, which can leak fluid or bleed under the macula. Symptoms include sudden central blurring, metamorphopsia and scotoma.
Treatment is primarily with intravitreal anti-VEGF injections. The American Academy of Ophthalmology notes that ophthalmologists have treated wet AMD with periodic eye injections and dry AMD with antioxidant vitamins for more than a decade.
Other High-Yield Retinal Conditions for PG Ophthalmology Exams
Central Retinal Artery and Vein Occlusion
Central retinal artery occlusion presents with sudden, painless, severe vision loss and a cherry-red spot at the macula. It is an emergency and requires systemic vascular evaluation.
Central retinal vein occlusion presents with sudden painless visual loss, dilated tortuous veins, widespread retinal haemorrhages and macular edema. Management depends on ischemic status, macular edema and neovascular complications.
Retinitis Pigmentosa: Genetic Basis and Clinical Findings
Retinitis pigmentosa is an inherited retinal dystrophy affecting photoreceptors. Classic features include night blindness, peripheral field constriction, waxy disc pallor, attenuated retinal vessels and bone-spicule pigmentation.
Residents must know inheritance patterns, ERG findings, visual field changes and counselling aspects.
Macular Hole and Epiretinal Membrane
Macular hole presents with central visual loss and metamorphopsia. OCT is the key investigation. Full-thickness macular holes may require vitrectomy with internal limiting membrane peeling and gas tamponade.
Epiretinal membrane causes retinal surface wrinkling, distortion and reduced vision. Surgical treatment is considered when symptoms or visual impairment are significant.
Vitreoretinal Surgery: What MD Ophthalmology Residents Need to Master
Vitreoretinal surgery is a key sub-speciality area after MD Ophthalmology. Even if a resident does not perform advanced surgery independently during residency, understanding the principles is essential.
Pars Plana Vitrectomy: Steps, Indications and Complications
Pars plana vitrectomy involves creating sclerotomies through the pars plana, removing the vitreous gel, treating retinal pathology, applying laser and using tamponade when needed. Indications include retinal detachment, vitreous haemorrhage, macular hole, epiretinal membrane, endophthalmitis, dropped nucleus and advanced diabetic eye disease.
Complications include cataract, retinal breaks, recurrent detachment, raised IOP, hypotony, infection and haemorrhage.
Small-Gauge Vitrectomy: 23G and 25G Systems in India
Small-gauge vitrectomy systems such as 23G, 25G and 27G allow smaller incisions, improved patient comfort and faster recovery in selected cases. Residents should understand the basic differences in wound construction, fluidics, instrumentation, illumination and surgical control.
Retina Fellowship After MD Ophthalmology: Scope in India
A retina fellowship after MD Ophthalmology is a strong option for residents interested in medical retina, surgical retina, diabetic eye disease, macular disorders, retinal imaging and vitreoretinal surgery. With increasing diabetic eye disease, ARMD, retinal vascular occlusions and trauma-related retinal conditions, trained retina specialists have wide scope in hospitals, institutes and private practice.
How DigiNerve’s Ophthalmology MD Course Covers Retinal Diseases
DigiNerve’s Online Ophthalmology MD course is designed to support MD Ophthalmology residents with structured learning across core and advanced topics. Retinal diseases are covered through expert-led video lectures, concept-focused explanations, clinical case-based learning, self-assessment questions and revision-friendly notes.
The course helps residents build clarity in high-yield retina topics such as diabetic retinopathy, retinal detachment, ARMD, retinal vascular occlusions, macular disorders and vitreoretinal surgery principles. With comprehensive video lectures, aligned digital notes, exam-oriented questions, benchmark trials, test series and Dr. Wise AI Chatbot, it supports both residency learning and university exam preparation.
Frequently Asked Questions
Q1. What are the most common retinal diseases tested in PG ophthalmology exams?
Ans – The most commonly tested retinal diseases include diabetic retinopathy, retinal detachment, age-related macular degeneration, retinal artery occlusion, retinal vein occlusion, retinitis pigmentosa, macular hole and epiretinal membrane.
Q2. What is the difference between tractional and rhegmatogenous retinal detachment?
Ans – Rhegmatogenous retinal detachment occurs due to a retinal break that allows fluid to enter the subretinal space. Tractional retinal detachment occurs when fibrovascular membranes pull the retina away, commonly in proliferative diabetic retinopathy.
Q3. Is vitreoretinal surgery covered in MD Ophthalmology residency in India?
Ans – Yes, MD Ophthalmology residents are expected to understand the principles, indications, steps and complications of vitreoretinal surgery. Advanced independent surgical training is usually pursued through a retina fellowship after residency.
Q4. Which fellowship is best after MD Ophthalmology for retina sub-speciality?
Ans – A vitreoretinal surgery fellowship or medical retina fellowship is best for residents who want to specialise in retinal diseases. The choice depends on whether the resident is more interested in retinal imaging and injections or advanced surgical retina procedures.