")
Ovulation Induction Protocols Explained (Clomiphene, Letrozole & Gonadotropins)
What is Ovulation Induction?
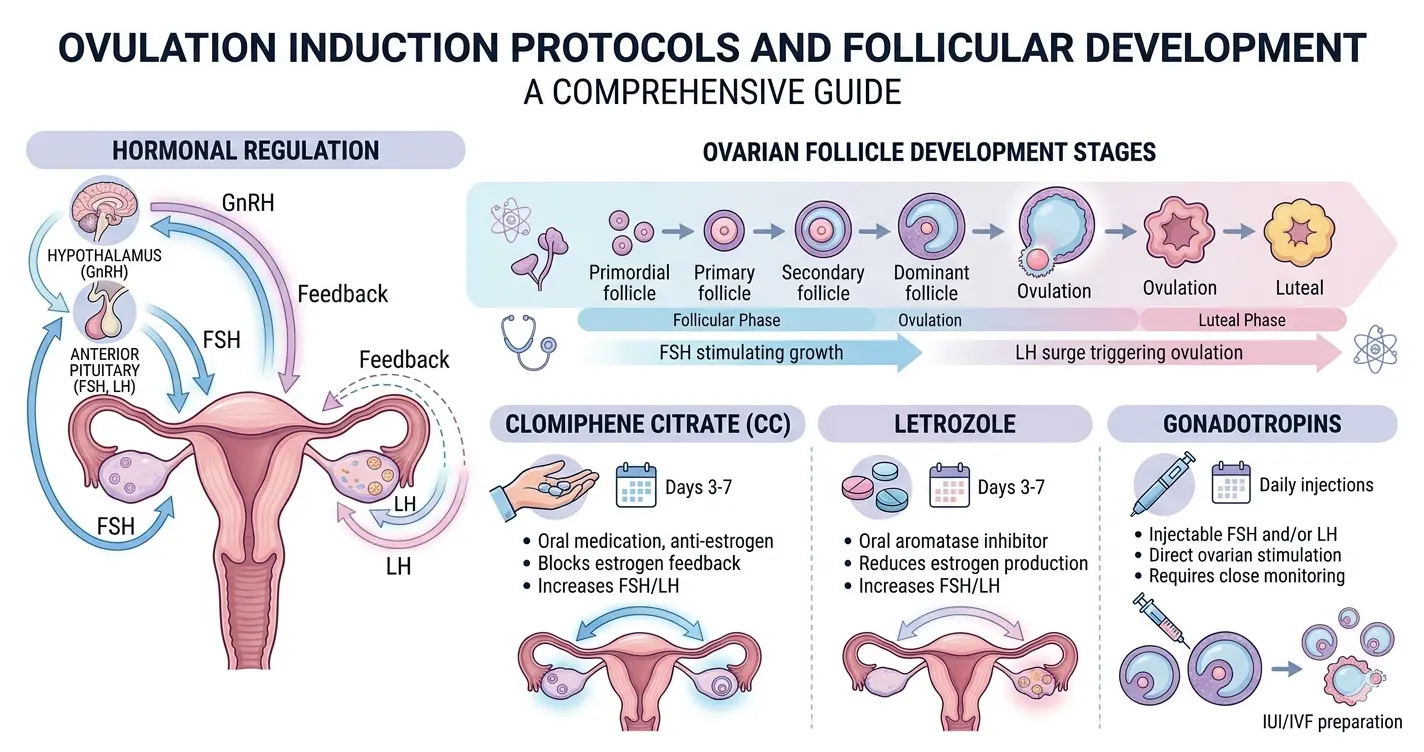 Ovulation induction refers to the pharmacological stimulation of ovarian follicular development to achieve ovulation in women with oligo-ovulation or anovulation. It involves targeted manipulation of the hypothalamic–pituitary–ovarian (HPO) axis, either by enhancing endogenous gonadotropin release or administering exogenous gonadotropins.
Ovulation induction refers to the pharmacological stimulation of ovarian follicular development to achieve ovulation in women with oligo-ovulation or anovulation. It involves targeted manipulation of the hypothalamic–pituitary–ovarian (HPO) axis, either by enhancing endogenous gonadotropin release or administering exogenous gonadotropins.
Physiologically, ovulation requires:
- Pulsatile GnRH secretion from the hypothalamus
- Release of FSH and LH from the anterior pituitary
- Follicular maturation and estradiol production
- Mid-cycle LH surge leading to ovulation
Disruption at any level of this axis can result in anovulation.
When is Ovulation Induction Used?
Ovulation induction protocols are indicated in:
- Chronic anovulation, especially in Polycystic Ovary Syndrome
- WHO Group II ovulatory dysfunction (normogonadotropic anovulation)
- Unexplained infertility
- Hypothalamic dysfunction (selected cases)
WHO classification (frequently tested concept):
- Group I: Hypogonadotropic hypogonadism
- Group II: Normogonadotropic (PCOS)
- Group III: Hypergonadotropic hypogonadism (ovarian failure)
Common Ovulation Induction Protocols
Clomiphene Citrate Protocol
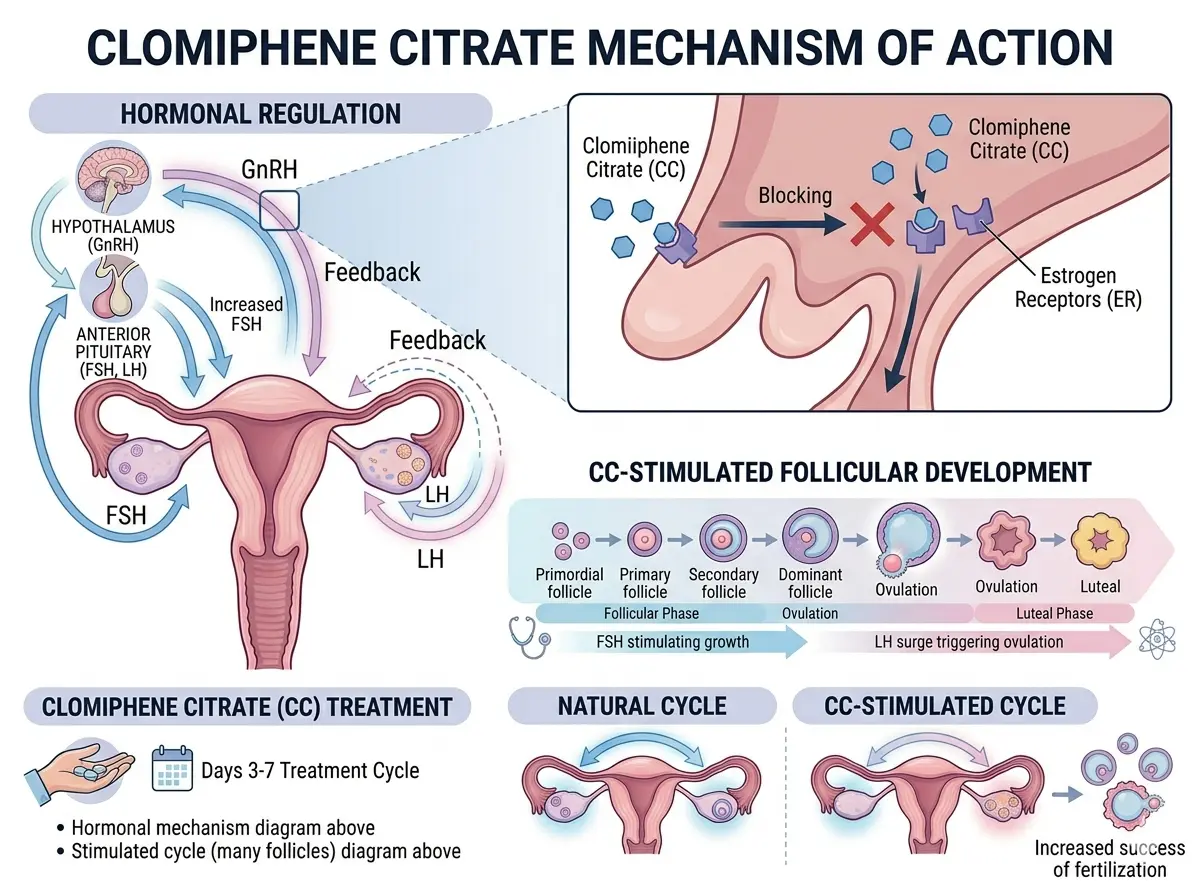 Drug Class: Selective Estrogen Receptor Modulator (SERM)
Drug Class: Selective Estrogen Receptor Modulator (SERM)
Clomiphene citrate mechanism:
- Competitive inhibition of estrogen receptors in the hypothalamus
- Removal of negative feedback → ↑ GnRH pulse frequency
- ↑ FSH and LH secretion → follicular recruitment
Standard Protocol:
- Initiation: Day 2–5 of the menstrual cycle
- Dose: 50 mg/day for 5 days
- Escalation: Up to 150 mg/day if no ovulation
Pharmacological Notes:
- Long half-life (~5–7 days)
- Anti-estrogenic peripheral effects
Limitations:
- Endometrial thinning
- Poor cervical mucus
- Risk of luteal phase defect
Letrozole Protocol
Drug Class: Aromatase inhibitor
Letrozole ovulation induction mechanism:
- Inhibits aromatase enzyme → ↓ conversion of androgens to estrogens
- Reduced estrogen levels → loss of negative feedback
- ↑ FSH secretion → folliculogenesis
Protocol:
- Initiation: Day 2–5
- Dose: 2.5–7.5 mg daily for 5 days
Pharmacodynamics:
- Short half-life (~45 hours)
- No persistent anti-estrogenic effect on the endometrium
Clinical Significance:
- Higher ovulation and live birth rates in PCOS
- Improved endometrial receptivity
Gonadotropin Protocol
Drugs Used:
- Recombinant FSH (rFSH)
- Human menopausal gonadotropin (hMG: FSH + LH activity)
Mechanism:
- Direct stimulation of ovarian follicles independent of hypothalamic-pituitary control
Protocols:
- Low-dose step-up: Gradual increase to avoid multifollicular development
- Step-down: High initial dose followed by reduction
Monitoring Requirements:
- Serial transvaginal ultrasonography
- Serum estradiol (E2) levels
Indications:
- Clomiphene-resistant anovulation
- Assisted reproductive techniques
Letrozole vs Clomiphene – Key Differences
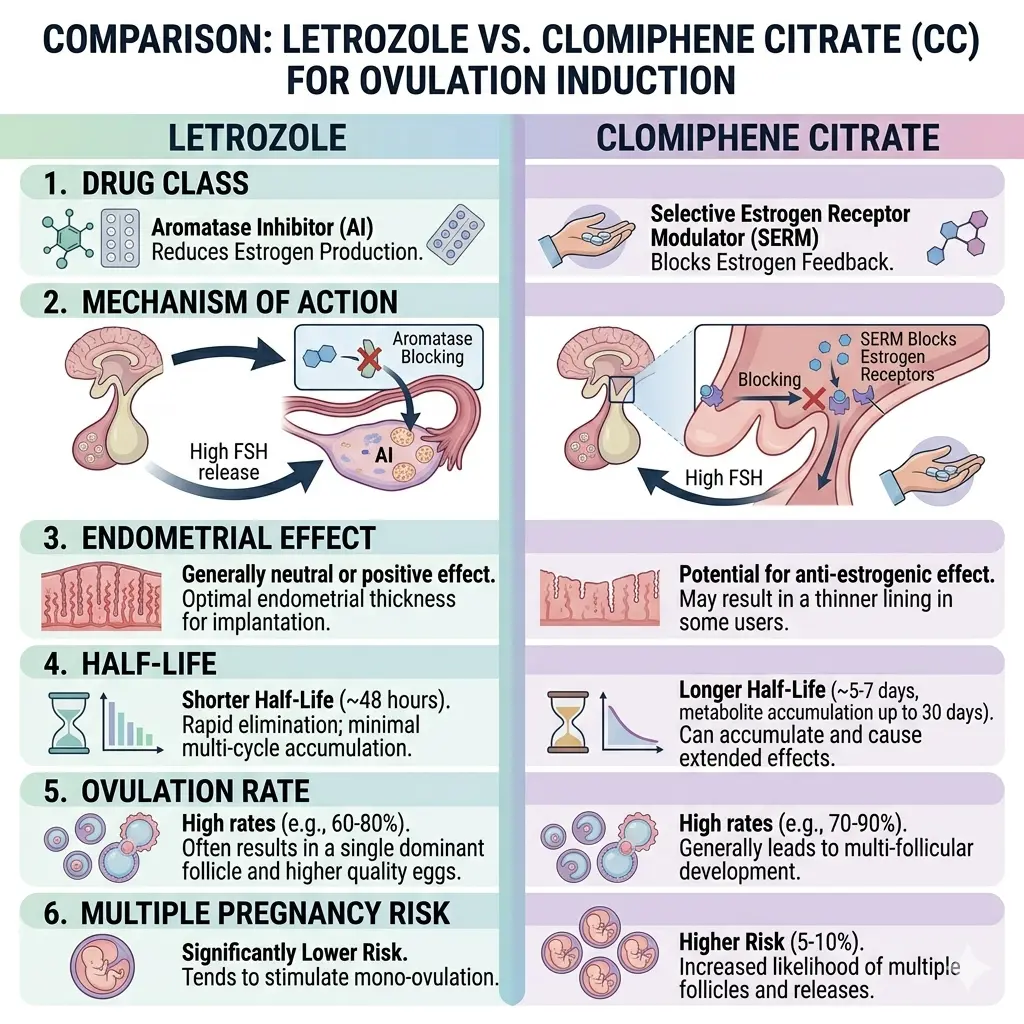
| Parameter | Letrozole | Clomiphene |
| Drug class | Aromatase inhibitor | SERM |
| Mechanism | ↓ Estrogen synthesis | Estrogen receptor blockade |
| Endometrial effect | Favorable | Anti-estrogenic |
| Half-life | Short | Long |
| Ovulation rate (PCOS) | Higher | Moderate |
| Multiple pregnancy risk | Lower | Higher |
The letrozole vs clomiphene comparison is clinically relevant, with letrozole now preferred in PCOS-related anovulation.
Types of Infertility Treatment Drugs
Ovulation induction drugs are categorised as:
- SERMs: Clomiphene citrate
- Aromatase inhibitors: Letrozole
- Gonadotropins: FSH, LH preparations
- Adjunct therapies:
- Insulin sensitisers (e.g., metformin)
- Luteal phase support (progesterone)
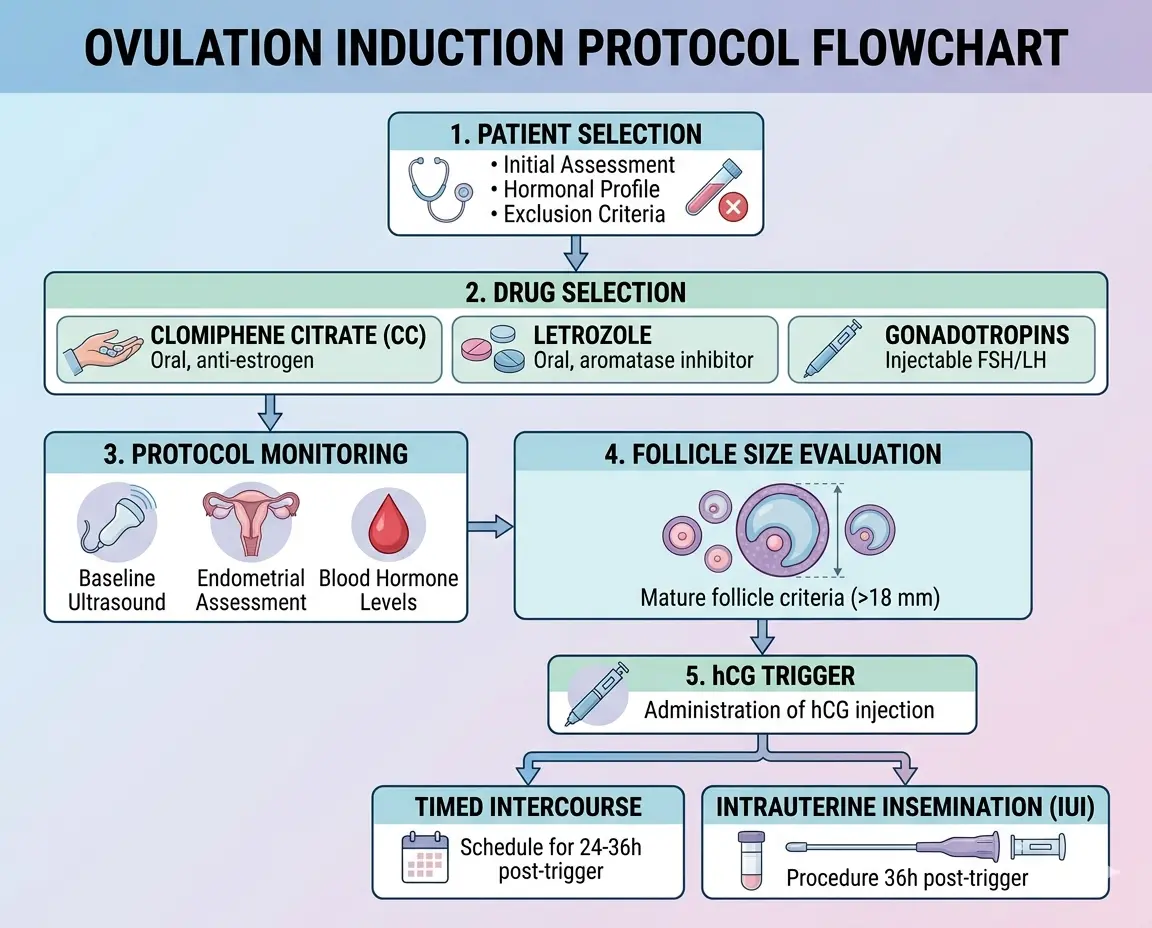
Step-by-Step Ovulation Induction Protocol
Patient Selection
- Confirm anovulation
- Assess ovarian reserve (AMH, AFC)
- Exclude:
- Tubal pathology
- Severe male factor infertility
Drug Selection
- PCOS → Letrozole
- General anovulation → Clomiphene/Letrozole
- Resistant cases → Gonadotropins
Monitoring
- Follicular tracking starting Day 9–10
- Dominant follicle: 18–20 mm
- Endometrial thickness: ≥7 mm
Trigger & Timing
- Administration of hCG trigger (mimics LH surge)
- Ovulation occurs ~36 hours post-trigger
- Timed intercourse or intrauterine insemination is planned accordingly
Risks and Complications
Ovarian Hyperstimulation Syndrome (OHSS)
- More common with gonadotropins
- Pathophysiology: Increased vascular permeability due to VEGF
- Features: Ascites, enlarged ovaries, hemoconcentration
Multiple Pregnancy
- Clomiphene: Increased twin rate
- Gonadotropins: Higher risk of multifetal gestation
Other Adverse Effects
- Functional ovarian cysts
- Vasomotor symptoms (clomiphene)
- Abdominal discomfort
Ovulation Induction in PCOS Patients
Key pathophysiology:
- Increased LH: FSH ratio
- Hyperandrogenism
- Arrested follicular development
Management principles:
- Letrozole as a first-line agent
- Lifestyle modification (weight reduction improves ovulation)
- Metformin in insulin-resistant individuals
Clomiphene resistance is defined as failure to ovulate at the maximum dosage.
Clinical Tips for Gynaecologists
- Aim for mono-follicular development to reduce complications
- Use the lowest effective dose
- Avoid excessive estradiol rise
- Individualise treatment based on ovarian reserve and BMI
Role of IUI in Ovulation Induction
Ovulation induction is frequently combined with intrauterine insemination to enhance conception rates.
- Indicated in unexplained infertility and mild male factor
- Synchronisation with ovulation improves fertilisation probability
High-Yield Revision Points
- Letrozole = Drug of choice in PCOS ovulation induction
- Clomiphene = SERM with anti-estrogenic effects
- Gonadotropins = Highest efficacy but highest risk (OHSS, multiples)
- Follicle size for trigger = 18–20 mm
- Clomiphene resistance = No ovulation at 150 mg dose
Ovulation induction protocols form a critical component of infertility management, integrating reproductive physiology with pharmacological intervention. A clear understanding of the clomiphene citrate mechanism, letrozole ovulation induction, and gonadotropin therapy infertility protocols is essential for clinical application and examinations. The transition toward letrozole as a preferred agent, particularly in PCOS, reflects evidence-based evolution in infertility treatment drugs.
NEET PG Pattern Questions:
Q1. The primary mechanism of action of clomiphene citrate is:
A. Direct ovarian stimulation
B. Aromatase inhibition
C. Estrogen receptor blockade in the hypothalamus
D. Progesterone receptor activation
Answer: C. Estrogen receptor blockade in the hypothalamus
Explanation: This increases GnRH secretion, leading to increased FSH and LH.
Q2. Ovulation trigger with hCG is usually given when the dominant follicle reaches:
A. 10–12 mm
B. 12–14 mm
C. 18–20 mm
D. 22–24 mm
Answer: C. 18–20 mm
Q3.Assertion (A): Letrozole is preferred over clomiphene in ovulation induction for PCOS.
Reason (R): Letrozole improves endometrial thickness compared to clomiphene.
- Both A and R are true, and R explains A
B. Both A and R are true, but R does not explain A
C. A is true, R is false
D. A is false, R is true
Answer: A. Both A and R are true, and R explains A
Q4. Clomiphene citrate is classified as:
A. Aromatase inhibitor
B. Selective estrogen receptor modulator
C. Progesterone analogue
D. GnRH analogue
Answer: B. Selective estrogen receptor modulator
Frequently Asked Questions:
Q1. What is the first-line drug for ovulation induction in PCOS?
Ans – Letrozole
Q2. What is the mechanism of clomiphene citrate?
Ans – Estrogen receptor blockade at hypothalamus → ↑ GnRH → ↑ FSH/LH
Q3. Define clomiphene resistance.
Ans – Failure to ovulate at 150 mg/day
Q4. What is the major complication of gonadotropin therapy?
Ans – Ovarian Hyperstimulation Syndrome (OHSS)
Q5. What is the ideal follicular size for an ovulation trigger?
Ans – 18–20 mm
Q6. Why is letrozole preferred over clomiphene?
Ans – Better endometrial effects and improved ovulation rates